
Advancing HealthTech for Humanity™
People shouldn’t have to reverse engineer their own medical devices. But, a lot of us do.
Medical device hardware and software has historically been very slow to evolve, but the non-medical technology available to an average person is now sufficient to encourage exploration of our medical devices. And many of us are unsatisfied with what we find.
How I started to exploring my own medical devices
I have lived with type 1 diabetes for more than 14 years. For the longest time, I accepted that there were critical flaws with the devices that were supposed to keep me alive. After all, I’m a patient – I’m supposed to be “patient” and wait for advancements in technology or a cure that are often promised to be “5 years from now”. But every night that I went to sleep, I was at risk of dying from hypoglycemia if I did not wake up to the alarms of my continuous glucose monitor. And the built-in device alarms were not loud enough to wake me up.
Frustrated, I accepted that I couldn’t change the physical medical device. But I knew that if I could somehow free my own data from the physical device, I could send it to my phone or any number of other devices where I could make the alarms louder. I didn’t have any way to do that until John Costik tweeted about pulling his son’s CGM data and sending it to the cloud. I asked John to share his code so I could do the same. This was my first exposure to open source and exploring my own medical devices, and I’ve been hooked ever since.
 I closed the loop – but it could have been easier
I closed the loop – but it could have been easier
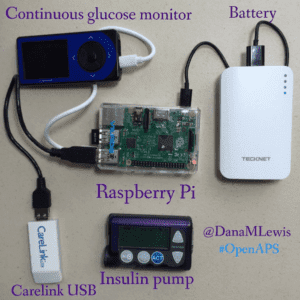
After creating a louder alarm system for myself, I iterated and built an algorithm that predicted the outcomes of certain actions that I would take that would influence my blood glucose levels. Essentially it was an “open loop”, although we just called it a “smart alarm” system at the time. Within a year, we realized that could be combined with Ben West’s years of work to decode communication with the insulin pump and enable a person to actually send commands remotely to the insulin pump. This is what enabled us to close the loop.
In one sense, closing the loop was ridiculously easy, especially since we had built and had been testing this algorithm for over a year. But, in another sense, looking at the years Ben spent figuring out the communication that the pump did, it WAS hard. And it continues to be hard for end users to reverse engineer and decode the communications of our medical devices. It definitely shouldn’t be this way.
 A call to action for standards and clearly documented communication protocols in medical devices
A call to action for standards and clearly documented communication protocols in medical devices
This is why we need standards. We need manufacturers to have something to lean on, to ensure that data is created by devices and accessible by users in a uniform way. We need to have clearly documented communication protocols for controlling our medical devices, rather than relying on security by obscurity, or locking down devices to prevent users from controlling them.
We are at the point where we patients have the same access to tools and technology as manufacturers and developers. Instead of being scared, manufacturers should look at this as an opportunity to get more real-time feedback and fixes to ultimately approve their devices and tools. This what the speed of evolving technology will enable – if healthcare and medical device manufacturers are willing to embrace it. This is the future, but it’s also possible today.
Dana Lewis is one of the founders of #OpenAPS, an open source movement to make artificial pancreas technology available more quickly. You can hear her talk about OpenAPS and open source in this OSCON keynote. For more about OpenAPS, check out www.OpenAPS.org.